AC Joint Injury
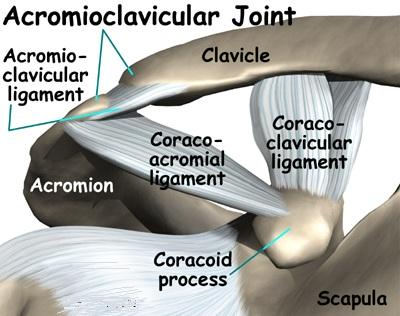
The Acromioclavicular Joint, or AC Joint is a joint at the top of the Shoulder. It is the junction between the Acromion (part of the scapula that forms the highest point of the shoulder) and the clavicle. It is a plane synovial joint.
Between the greater tubercle and the lesser tubercle is the intertubercular sulcus (bicipital groove).

Injury / Dislocation of AC Joint
The Acromioclavicular Joint is usually injured by a direct fall onto the point of the Shoulder. The Shoulder blade (scapula) is forced downwards and the clavicle (collarbone) appears prominent. The Acromioclavicular Joint is usually injured by a direct fall onto the point of the shoulder. The shoulder blade (scapula) is forced downwards and the clavicle (collarbone) appears prominent.
Types of Dislocations

Type 1
- Sprain of joint without a complete tear of either ligament
- There may be tenderness at the joint when touched.
- There may be some bruising around joint.
- There is minor pain with arm movement.
- There is no pain in the area of the coracoclavicular ligaments.

Type 2
Tear of AC Ligaments with coracoclavicular ligaments intact. Will not show marked elevation of lateral end of clavicle.
- There is moderate to severe pain at the joint.
- Swelling may be present.
- There is pain with arm movement.
- There may be a small bump on the top of the shoulder where the clavicle ends.
- The clavicle may move when pushed.
- The area of the coracoclavicular ligaments may be painful when touched.
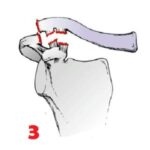
Type 3
In this injury both AC & CC ligaments are torn. 5 mm elevation of AC Joint without weights is consistent with severe type II or a type III injury.
- Typically, the injured person immediately supports the elbow while holding the arm close to the side. This prevents the pain outward arm movement would cause.
- Pain is present with any arm motion.
- Pain is present around the joint and in the area of the coracoclavicular ligaments.
- Swelling is present.
- As the joint moves, a popping sound may occur.
- There is shoulder deformity and a bump on the top of the Shoulder.
- The AC Joint is very unstable.

Type 4
Distal clavicle impaled posteriorly into trapezial fascia. This is a type III injury with avulsion of the coracoclavicular ligament. There is a tent in the posterior skin. This injury is generally requires a surgery.
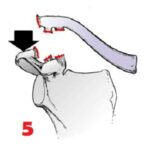
Type 5
Clavicle is markedly elevated and coracoclavicular distance is more than double than normal (e.g. >25mm) This is a more severe form of a type III injury, with the trapezial and deltoid fascia stripped off of the acromion as well as the clavicle. The shoulder manifests as a severe droop, secondary to downward displacement of the scapula and humerus due to loss of the clavicular strut. This injury generally requires surgery.
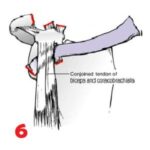
Type 6
Clavicle inferiorly displaced behind coracobrachialis and biceps tendons. Most patients with type VI injuries have paresthesia that resolves after relocation of the clavicle. It is extremely rare and generally only involved with motor vehicle collisions. This requires surgery.
Investigations:
- X-Ray to know status of joint.
- MRI to show status of Ligaments.


Treatment:
Non-operativeTreatment :
Type 1 to type 3 injuries are treated successfully with non-operative treatment that may include :
- Ice to reduce pain and swelling.
- Rest and a protective sling until pain subside.
- Anti-inflammatory medications.
This usually takes about 1-2 weeks A rehabilitation program to restore normal motion and strength is begun as soon as tolerated with gentle exercises and progresses as healing allows.
Depending upon the grade of injury, most patients heal within 2 to 3 months without surgical intervention.
The patient is allowed to return to sports when there is full and painless range of motion, no more tenderness when the AC joint is touched and manual traction does not cause pain. This usually takes about 2 weeks for a grade I injury, 6 weeks for a grade II injury, and up to 12 weeks for a grade III injury.
Operative Treatment:
Surgery may be necessary for AC separations that do not respond well to non-operative treatment or type 4 to type 6 injuries. If, after 2 to 3 months, pain continues in the AC Joint with overhead activity or in contact sports, surgery may be necessary.These patients include:
- Young, active individuals (over the age of 13).
- Laborers whose jobs require heavy overhead work.
- Athletes in non-contact sports whose overhead movements are stressful and frequent.
A variety of surgical methods have been used to stabilize a separated AC Joint. The surgical technique most often performed involves the reconstruction of the coracoclavicular ligaments and the excising (removal) of the distal (shoulder) end of the clavicle. Distal clavicle resection without the repair of the ligaments may lead to excessive rotation of the scapula. Reconstruction studies show that the AC Joint can be adequately stabilized by :
- A fixation across the acromioclavicular space with pins or plates.
- Loop fixation from the clavicle to the coracoid process using synthetic materials.
- The most common reconstructive procedures of today use a screw or suture loop to stabilize the joint.
In a distal clavicle resection, about 10-15mm of the clavicle is removed through a two-inch incision above the joint. The AC Ligament is then transferred from the bottom of the acromion into the cut end of the clavicle to replace the torn ligament.
Contact us
Make an Appointment
Contact
+ 91 9760070333
Location
Verman Hospital,Sadar Road,Mathura,281001